

-
Coordination of Benefits (COB)
The Coordination of Benefits (COB) provision applies when a person has health care coverage under more than one plan. The order of benefit determination rules govern the order in which each plan will pay a claim for benefits. The plan that pays first is called the primary plan. The primary plan must pay benefits in accordance with its policy terms without regard to the possibility that another plan may cover some expenses. The plan that pays after the primary plan is the secondary plan. The secondary plan may reduce the benefits it pays so that payments from all plans does not exceed 100% of the total allowable expense.
*Disclaimer: Coordination of Benefits does not apply to enrollees in Tennessee.
-
Cost estimator tool
As of January 1, 2023, plans and issuers must make price comparison information available with respect to an initial list of 500 identified items and services. By January 1, 2024, plans and issuers must make price comparison information available with respect to all covered items and services. You must be logged into the member portal in order to use the estimator tool. Click here to access the member portal.
-
Information of Explanation of Benefits (EOB)
An EOB is a helpful tool for keeping track of your Ascension Personalized Care healthcare benefits. It shows you how your health plan processed a healthcare claim. EOBs look similar to a bill, but they function differently. The EOB will be in the form of a letter that includes a chart showing how your claim was processed. Always check your EOB, and make sure the information displayed is accurate. If any information is missing or if you have questions regarding your EOB, contact the customer service number located on the back of your member ID card.
See the list below of key elements included in your EOB:
- Name of patient: Make sure your name or the name of another person who is covered by your health plan is displayed on the EOB.
- Insured ID number: This should match the number on your member ID card.
- Claim number: The number by which you and your health plan will be able to refer to a claim should you have questions or concerns.
- Provider: The name of the healthcare provider who provided this service. This could be the name of a specific doctor, or of a hospital or other location.
- Date of service: The start and end date of the service.
- Type of service: A description of the service received.
- Healthcare provider charge: The amount billed to your health plan by the healthcare provider.
- Cost covered by your health plan: The total your health plan paid for your services.
- What you owe: Any balance the healthcare provider billed that was not covered by your health plan.
-
Machine-readable files
In order to comply with the Transparency in Coverage legislation, insurance plans are required to make available machine-readable files for in-network rates (for doctors in the plan's network) and for out-of-network rates (for doctors not in the plan's network). Select the desired file for more information.
Please note: These files contain a large amount of data and my require several minutes to download/open.
June 2025 in-network rates - Indiana
June 2025 in-network rates - Kansas
June2025 in-network rates - Michigan
June 2025 in-network rates - Tennessee
June 2025 in-network rates - Texas
-
Medical necessity and prior authorization
A prior authorization is an approval from your health plan. It may be required before you are able to fill a prescription or receive a medical service. Please call us at 844-995-1145 to obtain a prior authorization.
Prior authorization review is intended to confirm the medical necessity, as defined in your policy, of a setting, service, treatment, supply, device, or prescription drug. If a setting, service, treatment, supply, device, or prescription drug is listed below, prior authorization review must be obtained before incurring any claims for that setting, service, treatment, supply, device, or prescription drug. You are responsible for obtaining prior authorization review when required. You can obtain prior authorization review by contacting us at:
Seton Health Plan Medical Management
1345 Philomena St., Suite 305
Austin, TX 78723
Phone: 844-995-1145
Fax: 512-380-7507
Email: SHP-Authorization@ascension.org
Prior authorization is not a guarantee that benefits will be payable. All benefits payable are subject to all of the terms, conditions, provisions, exclusions, and limitations of the Policy.
The following settings, services, treatments, supplies, devices, or prescription drugs require prior authorization review:
- Inpatient admissions (including acute care, long term acute care- behavioral health and/or substance abuse use disorder
rehabilitation, residential treatment and partial hospitalization; skilled nursing facility). - Emergency admissions within 48 hours following admission
- High risk maternity (routine that exceeds federal requirements)
- Outpatient surgical procedures
- Oral pharynx procedures
- Spinal procedures
- Diagnostic radiology
- Therapeutic radiology
- Neuropsychological testing
- Orthotics and prosthetics
- Durable medical equipment (including DME items more than $1000)
- Hearing (EAR) devices
- Transplants (other than corneal transplants)
- Home health care
- Home infusion therapy
- Rehabilitative and habilitative outpatient therapy
- Injectable medications (administered by a healthcare doctor)
- Genetic testing
*Potential experimental or investigational treatment, testing or procedures
*List of services requiring prior authorization is not all inclusive.
Failure to utilize or abide by the decisions of the Utilization Management Program will result in the denial of the claim for failing to prior authorize in advance of the proposed procedure or admission. Disclaimer: Due to Texas Department of Insurance rules, Texas members will receive a reduction in benefits up to 50% of the allowable charge.
- Inpatient admissions (including acute care, long term acute care- behavioral health and/or substance abuse use disorder
-
Member claims submissions
Ascension Personalized Care in-network plan doctors file claims for members after they receive services. Claim forms can only be submitted to Ascension Personalized Care by doctors for Ascension Personalized Care members.
To contact customer service, please call 833-600-1311.
-
Member complaints, grievances, and appeals - Medical
We have steps for handling any insurance-related problems you may have. To keep you satisfied, we provide processes for filing appeals or complaints. You have the right to file a complaint, file an appeal, and have an external review. We hope you will always be happy with our doctors and us. But if you aren’t, or you aren’t able to find answers to your questions, we have steps for you to follow:
- Inquiry process
- Complaint process
- Grievance process
- Appeal process
- External review by an independent review organization (IRO)
- Complaint to your state’s insurance department: Kansas Insurance Department, Indiana Department of Insurance, Tennessee Department of Commerce and Insurance, or Texas Department of Insurance
Your satisfaction is very important to us. We want to know your issues and concerns so we can improve our services. Please contact our Member Services team at 833-600-1311 Monday through Friday, 8:00 a.m. to 6:00 p.m. EST., TTY: 586-693-1214 or you can email us at apcsupport@ascension.org. We will attempt to answer your questions during initial contact, as most concerns can be resolved with one phone call. The following processes are available to address your concerns:
How to file an inquiry
An inquiry is a request for clarification of a benefit, product, or eligibility where no expression of dissatisfaction is made. Examples of an inquiry are:- How to make a payment
- How to find a doctor or change primary care provider
- Billing questions
- Premium questions
- How to find a Member ID
How to file a complaint
A complaint is an oral expression of dissatisfaction. Some complaints can be resolved through a phone call. Some examples include:
- Length of time to see a doctor
- Can’t find a doctor or they are not accepting new patients
- Multiple customer service interactions and the issue is still not resolved
- Trouble enrolling on the website
- Need help locating information on the website
- Doctor and/or staff were rude
To file a complaint, call member services at 833-600-1311 Monday through Friday, 8:00 a.m. to 6:00 p.m. EST., TTY: 586-693-1214. For a full list of definitions, please refer to your Evidence of Coverage.
How to file a grievance
A grievance means any dissatisfaction with an insurer offering a health benefit plan or administration of a health benefit plan by the insurer that is expressed verbally, or in writing in any form to the insurer by, or on behalf of, a claimant including any of the following:- Providing of services
- Determination to rescind a policy
- Determination of a diagnosis or level of service required for evidence-based treatment of autism spectrum disorders
- Claims practices
- Cancellation of your benefit coverage with us
Examples of a grievance would be:
- Generic prescription didn’t have the generic copay applied
- Preventive procedure was not covered at 100%
- Need a case coordinator to contact me regarding home healthcare
- Consent issues
- Allergic reaction to prescribed medication
- Plan coverage concerns
To file a grievance, call Member Services at 833-600-1311 Monday through Friday, 8:00 a.m. to 6:00 p.m. EST., TTY: 586-693-1214.
You may file a grievance verbally, or in writing, either by mail or by email at apcsupport@ascension.org. If you require assistance in filing a grievance or if you are unable to submit the grievance in writing, you can call Member Services at 833-600-1311 (TTY: 586-693-1214) to ask for help through the process. We will send a grievance acknowledgment letter after receipt of your grievance.
Send your written grievance form to:
US Health and Life Insurance Company
PO Box 1707
Troy, MI 48099-1707Expedited grievance: If your grievance concerns are an emergency or a situation in which you may be forced to leave the hospital prematurely, or if a standard resolution process will risk serious jeopardy to your life, pregnancy, or health.
Standard grievance: A grievance that does not meet the expedited definition of grievance.
View your Evidence of Coverage for full complaint procedures and processes, including specific filing details and time frames. You can access your Evidence of Coverage in your online member account. You may also file a grievance with the Department of Insurance.
How to file an appeal
An appeal is a request to reconsider a decision about the member’s benefits where either a service or claim has been denied. A denial includes a request for us to reconsider our decision to deny, modify, reduce, or terminate payment, coverage, authorization, or provision of healthcare services or benefits, including the admission to, or continued stay in, a healthcare facility. Failure to approve or deny a prior authorization request in a timely manner may be considered as a denial and subject to the appeal process. Examples of an appeal are:- Access to healthcare benefits, including an adverse determination made pursuant to utilization management
- Admission to or continued stay in a healthcare facility
- Claims payment, handling, or reimbursement for healthcare services
- Matters pertaining to the contractual relationship between a member and Ascension Personalized Care
- Cancellation of benefit coverage
- Other matters as specifically required by state law or regulation
To file a written appeal, you can mail or email your request to us:
US Health and Life Insurance Company
PO Box 1707
Troy, MI 48099-1707
apcsupport@ascension.org
Resolution time frames may vary based on the type of appeal filed. Please see Evidence of Coverage for details.
Expedited appeal: If your appeal concerns an emergency or a situation in which you may be forced to leave the hospital prematurely, or if you believe a standard resolution process will risk serious jeopardy to your life, pregnancy, or health.
Standard appeal: An appeal that does not meet the expedited definition.
How to request an external review
Once all appeal methods described above and of which are available within this health plan have been exhausted, you may request an external review from the state insurance department. You or your authorized representative will send a written request for this external review with the required forms that we have provided to you to the state department where you reside. The department will determine if your request qualifies for an expedited review and if it does, they or we (based on your state’s laws) may assign it to an Independent Review Organization (IRO).
When you file an external review under this health plan, you will not be subject to retaliation for exercising this right; you are permitted to utilize the assistance of other individuals, including health care doctors or providers, attorneys, friends, and family members throughout the review process; you are permitted to submit additional information relating to the proposed service throughout the review process; and you must cooperate with the IRO by providing any requested medical information or authorizing the release of any necessary medical information.The IRO will conduct a review and provide their recommendation to the department. The department will provide you with the decision within 72 hours for expedited external review after your request for an external review is filed; or within 15 days after your filing of a request for external review following a standard appeal. The decision made by the department will be final under the Patient’s Right to Independent Review Act of 2000.
Write to the appropriate state listed below to request an external review as described above; or to file your complaint:
Members in the state of Indiana:
State of Indiana Department of Insurance
Consumer Services Division
311 West Washington Street
Suite 300
Indianapolis, IN 46204
Consumer Hotline: 800-622-4461 or 317-232-2395
Online: in.gov/idoi/consumer-services/
Attn: Consumer Insurance Services
Members in the state of Kansas:
Kansas Insurance Commissioner
Kansas Insurance Department
1300 SW Arrowhead Road
Topeka, KS 66604
Phone: 785-296-3071 or 800-432-2484
Members in the state of Tennessee:
500 James Robertson Pkwy, 10th Floor
Nashville, TN 37243
Phone: 800-342-4029 or 615-741-2218
Online: tn.gov/commerce/insurance/consumer-resources/file-a-complaint.html
Members in the state of Texas:Texas Department of Insurance (TDI)Phone: 888-834-3476 or 512-322-3400 (Austin area)
-
Member complaints, grievances, and appeals - Prescription Drugs
MaxorPlus’ National Appeals Policy consists of a single-level internal appeals process for resolving disputes regarding pre/post-service medical necessity denials of covered benefits, as well as post-service benefits coverage denials. If an issue cannot be quickly resolved prior to appeal, a formal internal appeals process can be initiated in writing, usually up to 180 calendar days from the date of last determination.
In each case, MaxorPlus may be entitled to a one-time extension of not more than 15 days. Expedited appeals are conducted within the timeframe limits required by applicable state and federal regulations.
Reviewers making appeal determinations are selected to assure that neither they nor their managers were involved in the prior decision.
To submit an appeal for a prescription drug (Rx) to MaxorPlus:
• Fill out the Rx Appeal Filing Form for Ascension Personalized Care.
• Once the Appeal Filing Form is filled out, please fax to the number below:
• Standard Rx appeals fax number APC: 844-370-6203
• Expedited Rx appeals fax number APC: 844-370-6203
• Appeal Filing Form can be mailed to: MaxorPlus Clinical Department 320 S. Polk St., Amarillo, TX 79101
• If you wish to speak with someone regarding status of an appeal, the phone number is 888-839-4448
-
Member recoupment of overpaymentsMembers can dispute premium charges or payments by contacting customer service at 833-600-1311.
-
Nonpayment of premium and grace period for premium tax credits
Members must pay all monthly premiums to Ascension Personalized Care when they are due. If payments are late, Ascension Personalized Care will provide a notice to members with information on how to keep coverage. This includes paying all premiums owed by the end of the grace period as defined below.
For members not receiving advanced premium tax credits (APTC), Ascension Personalized Care provides a grace period of 30-days for payment of monthly premiums (this does not include the first binder premium payment). Coverage will continue during the 30-day grace period. If Ascension Personalized Care does not receive the entire premium amount that is due by the end of the grace period, coverage will be cancelled back to the last day of the grace period. Members may be responsible to Ascension Personalized Care for the payment of the portion of the premium for the time coverage was in effect during the grace period.
For members receiving an APTC, Ascension Personalized Care provides a grace period of 90-days if the member has previously paid at least one full month’s premium during the benefit year. During the grace period Ascension Personalized Care will:
- Pay all appropriate claims for services rendered to the member during the first month of the grace period and may pend (hold) claim payment for services rendered to the member in the second and third months of the grace period;
- Notify Health and Human Services (HHS) of such non-payment; and
- Notify doctors of the possibility of denied claims when a member is in the second and third months of the grace period.
If a member receiving APTC reaches the end of their 90-day grace period without paying all outstanding premiums, we will notify the member that coverage will be cancelled. The last day of coverage will be the last day of the first month of the 90-day grace period. Members will be responsible for payment of all charges for claims that were pended or paid during the second and third month of the grace period.
-
Out-of-network services and balance billing
To receive benefits from coverage, members must use a network doctor. However, payment will be made at the network doctor level of benefits for services provided by an out-of-network doctor when the services are provided for a medical emergency. Ascension Personalized Care will provide the member with listings of in-network doctors in the Ascension Personalized Care service area. The member is responsible for choosing their doctors for health care services.
For covered emergency services, members will pay in-network cost sharing (copayment, coinsurance and deductible). Members will also pay in-network cost sharing for services provided by some out-of-network doctors (such as anesthesiologists or pathologists) that provide services at a network hospital or if the out-of-network doctor provides certain services at in a network hospital or facility and does not notify the member of their out-of-network status. These out-of-network doctors are also prohibited from billing the member for any amounts in excess of the member’s cost sharing responsibility.
-
Prescription drug exception and expedited processDoctors or members may request and gain access to a drug not on the plan’s formulary under certain situations. The member’s doctor may recommend a particular service or FDA-approved item based on a determination of Medical Necessity with respect to that individual. To apply for an exception the claim must first be denied and then an exception appeal can be processed. Under this process, we will notify the member, the Insured’s designee and physician of our decision within 72 hours after we receive the exception request. The member or the member’s designee/doctor may request an expedited exception based on exigent circumstances and receive notification no later than 24 hours after making the request.
The member or doctor can submit the drug exception request to MaxorPlus by faxing the Rx Appeal Filing Form to 844-370-6203 or mailing to the address listed on the form. To request an expedited review for exigent circumstance, contact MaxorPlus' customer service department at the toll-free number listed on the back of your ID card to begin the process.
-
Prescription drugs requiring a prior authorization
Coverage for certain prescription drugs and related supplies requires your doctor to obtain authorization prior to prescribing. Prior authorization may include, for example, a Step Therapy determination. Step Therapy determines the specific usage progression of therapeutically equivalent drug products or supplies appropriate for treatment of a specific condition. If your doctor believes non-Prescription Drug List prescription drugs or related supplies are necessary, or wishes to request coverage for prescription drugs and related supplies for which prior authorization is required, your doctor may call or complete the appropriate prior authorization form and fax it to MaxorPlus to request a Prescription Drug List exception or prior authorization for coverage of the prescription drugs and related supplies. Your doctor should make this request before writing the prescription.
If the request is approved, your doctor will receive confirmation. The authorization will be processed in our claim system to allow you to have coverage for those prescription drugs and related supplies. The length of the authorization will depend on the diagnosis and prescription drugs and related supplies. When your doctor advises you that coverage for the prescription drugs and related supplies has been approved, you should contact the pharmacy to fill the prescription(s).
If the request is denied, your doctor and you will be notified that coverage for the prescription drugs and related supplies is not authorized. If you disagree with a coverage decision, you may appeal that decision in accordance with the provisions of the policy, by submitting a written request stating why the prescription drugs and related supplies should be covered.
If you have questions about a specific Prescription Drug List exception or prior authorization request, you should call Customer Service at the toll-free number on the back of your MaxorPlus ID card. All third-party review processes are handled by Ascension Personalized Care.
-
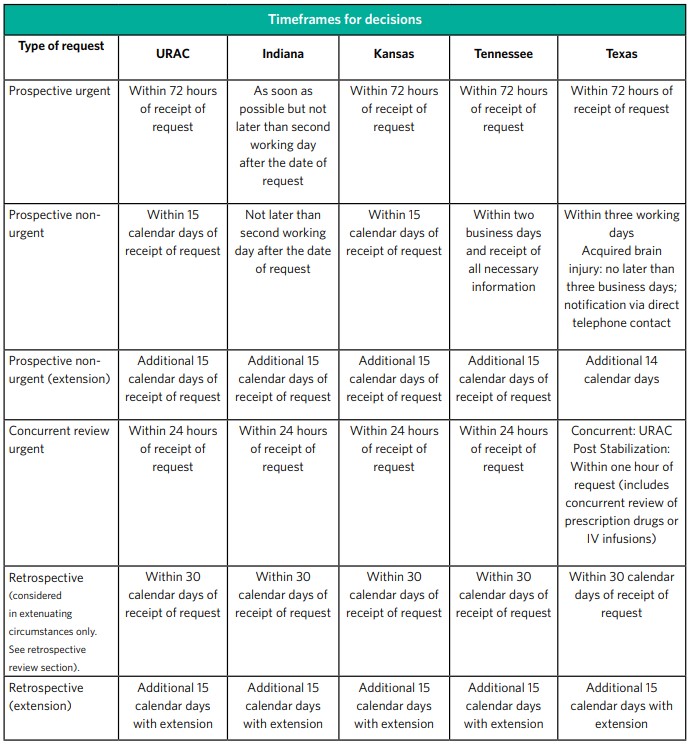
Prior authorization timeframe
Pre-certification determinations are made according to the URAC time standards.
Note: Where state or federal time standards differ from URAC, the more stringent time standard is applicable.
Standard organization determinations
Standard organization determinations are made as expeditiously as the member’s health condition requires, but no later than 15 calendar days after we receive the request for service. Please note that when state or federal time standards differ, the more stringent time standard is applied. An extension may be granted for 14 additional calendar days if the member requests an extension, or if we justify the need for additional information and documents that the delay is in the best interest of the member.
Expedited organization determinations
Expedited organization determinations are made when the member or their clinician believes that waiting for a decision under the standard timeframe could place the member’s life, health or ability to regain maximum function in serious jeopardy. The determination will be made as expeditiously as the member’s health condition requires, but no later than 72 hours after receiving the member or clinician’s request. Please note that when state or federal time standards differ, the more stringent time standard is applied. An extension may be granted for 14 additional calendar days if the member requests an extension, or if we justify a need for additional information and document how the delay is in the best interest of the member. Expedited organization determinations may not be requested for cases in which the only issue involves a claim for payment for services that the member has already received. Expedited urgent requests must be called to Ascension Personalized Care phone at 844-995-1145.
-
Retroactive denial of claims
A retroactive denial is the reversal of a claim we've already paid. If we retroactively deny a claim we have already paid for you, you are responsible for payment. Some reasons why you might have a retroactive denial include:
- Having a claim that was paid during the second or third month of a grace period
- Having a claim paid for a service for which you were not eligible.
You can avoid retroactive denials by paying your premiums on time and in full, and making sure you talk to your doctor about whether the service performed is a covered benefit. You can also avoid retroactive denials by obtaining your medical services from an in-network doctor.
If You or the Responsible Adult fails to pay the required premium, for individuals receiving advance premium tax credits, we will continue to pay all appropriate claims for covered services rendered to the enrollee during the first month of your three month grace period and pend claims for the second and third month of the grace period. For individuals with policies issued in the state of Texas and receiving advance premium tax credits, we will pay all appropriate claims for the entire three month grace period. We will notify HHS of the non-payment of premiums, the enrollee, as well as providers of the possibility of denied claims. We will continue to collect advanced premium tax credits on behalf of the enrollee from the Department of the Treasury, and will return the advanced premium tax credits on behalf of the enrollee for the second and third month of the grace period if the enrollee exhausts their grace period as described above. An enrollee is not eligible to re-enroll once terminated, unless an enrollee has a special enrollment circumstance, such as a marriage or birth in the family or during annual open enrollment periods.
If You or the Responsible Adult fails to pay the required Premium within the grace period, and you do not receive advance premium tax credits, your policy may likely terminate retroactively back to the last day of the month in which Premiums were paid for your coverage. If you are an individual receiving advance premium tax credits, your policy will likely terminate at the end of the first month of our grace period. You will be responsible for paying any claims related to services provided and submitted during the grace period and subsequent to any termination effective date if this plan terminates. Where allowed by state law, we will pend claims during the grace period and providers may call our offices to inquire about payment. We will advise them that the claims are pended and the providers may reach out to you for payment.
If you need to understand the terms of your plan and the grace period for your plan, we strongly encourage you to call and speak to our Customer Service team to outline your payment options to avoid termination of coverage.
We appreciate your business and we are committed to helping you in your healthcare journey.